Review of the literature by Valerie Dowley, Independent Tissue Viability Specialist. October 2023.
Quick refresh, what is MASD and why all the fuss?
Moisture Associated Skin Damage (MASD) is an umbrella term for skin inflammation or skin erosion caused by prolonged exposure to a source of moisture such as urine, sweat, faeces, wound exudate, saliva, or mucus (LeBlanc, 2019). There are 4 main types of MASD which are.
- Intertriginous Dermatitis (ITD) which is where moisture gets trapped within folds of skin causing inflammation.
- Peristomal MASD – inflammation and erosion, caused by moisture, around and extending outwards from the stoma/skin junction.
- Peri-wound MASD – skin maceration and erosion from wound exudate.
- Incontinence Associated Dermatitis (IAD) – chemical irritation caused by prolonged contact between the skin and urine and/or faeces. (Fletcher, J. 2020. Yates, A, 2020)
For the purposes of this clinical blog, I am going to discuss the final 2 distinct conditions under the umbrella of MASD. Peri-wound and Peristomal Moisture Associated Dermatitis.
Peri-wound Associated Dermatitis
The peri-wound area is defined as any skin within 4cm of the edge of a wound as well as any normal skin contained under a dressing (Dowsett et al, 2015a). Peri-wound moisture-associated dermatitis is often referred to as maceration.
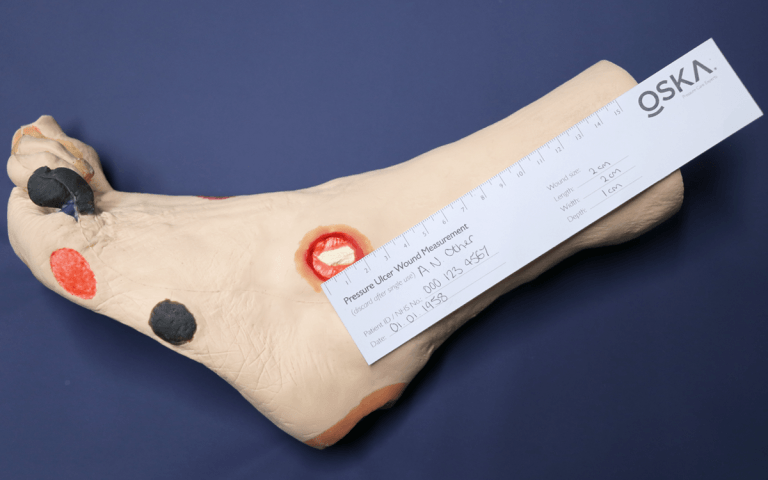
Maceration is caused when excessive amounts of wound exudate sit on the normal skin around a wound and causes this tissue to become overhydrated (macerated), boggy and may even breakdown. Peri-wound skin affected by maceration usually appears white in colour (Hollaway 2020). This excessive exudate increases the risk of the healthy peri-wound skin breaking down as it affects the skin barrier function, causes over hydration of the epidermal layer and can increase skin sensitivities that can lead to contact dermatitis.

Figure 1. Macerated Foot
Excoriation is a term used to describe a situation where lengthy exposure to wound exudate, which contains protease enzymes, eats away at the upper layers of the epidermis causing stripping of the skin. This is again due to excessive and unmanaged wound exudate and often follows a period of peri-wound maceration. It is preventable if the wound exudate is managed well with frequent dressing changes and the use of appropriate and effective super-absorbent dressing pads.
How to manage Peri-wound Moisture-Associated Dermatitis
Management of the peri wound skin is important to avoid the risk of maceration and excoriation and should be based on an accurate wound assessment, diagnosis of the cause of excessive moisture and a care plan put in place to manage this (Dowsett and Allen, 2013). These should include.
- Treat the underlying cause. What is causing the excessive exudate?
- Are the dressings being changed often enough? Is the dressing pad soaked when it is time to do the dressing change?
- Does the wound need debriding of devitalised tissue to reduce the bacterial burden and improve the wound environment?
- Is there oedema to the legs which is leaking out through the broken skin? Does the patient get effective leg elevation? Do they need to be assessed for compression bandages?
- Is there evidence of a wound infection that is untreated causing the excessive exudate?
- Cleaning the skin and implementing a structured skin care regime. This should include the use of skin barrier products or emollients. The patient should be involved in the decision-making process.
- Avoid using adhesive tapes and dressings if the skin is excoriated. Consider using silicone adhesive with high-risk patients or those with fragile skin. Could you use cotton stockinette and a tubular bandage instead to hold dressings in place?
- Is the skin dry? Dry skin can lead to bacterial skin infections due to damaged skin integrity. Regular use of emollients to prevent skin dryness. Emollients that contain Petroleum (Paraffin) can create an occlusive and protective layer on the skin and increase skin hydration but should be used with caution. Paraffin based products have a high flammability index and a risk assessment should be carried out especially if the patient is a smoker (Hollaway 2020).
Peristomal Dermatitis
Peristomal dermatitis is defined as inflammation and erosion of the skin relating to moisture that begins at the stoma/skin junction and can extend outwards in a 4-inch radius (Colwell et al 2011).
Skin disorders are a common problem for patients with stomas and 50% of these are because of irritant contact dermatitis. This is not surprising due to the unnatural apposition of bowel with abdominal skin which is not adapted to being in repeated contact with urine or faeces (Al-Niaimi, 2012). The most common sources of moisture are urine or faeces but other factors such as sweat, perspiration, external water sources (bathing and swimming) or wound drainage may also be causative factors needing to be considered. The main ingredient in the stoma product adhesive flanges is Hydrocolloid, which can absorb a certain amount of moisture, but if the moisture level is excessive then this barrier erodes and loses its protective function, allowing the irritants to sit on the skin and damage the skin integrity.
How to manage Peri-stomal Dermatitis
The management of the peri stomal dermatitis should initially focus on the affected skin, location of damage skin, and determining the source of the irritant. These should include:

Figure 2. Peri-stomal Dermatitis
- Treat the underlying cause. What is causing the skin irritation?
- What products are being used (barrier paste, skin protectant and cleansing method)? Do these meet the needs of the patient and fluid output?
- Where is the stoma sited? Is it within a skin fold? Has the patient gained or lost weight? Is there a peristomal hernia? How does the stoma sit when the patient is in various positions such as sitting, lying, standing and is this part of the problem?
- Is the removal process causing skin stripping (maybe changing bag too frequently, or using irritant products to help remove flange).
- Is the patients pouch application method good? Are they lining up the stoma and pouch opening well? Is the fit good or are there gaps between the pouch opening and the stoma allowing urine or faeces to sit on the skin?
- Is the skin damage a reaction to the products being used (allergic contact dermatitis)?
- Cleaning the skin around the stoma with a pH balanced product or water only, using a cotton wipe. If a cleanser is used, it should be rinsed away thoroughly avoiding oily or perfumed products.
- Make sure the skin is dried completely to avoid fungal infections and obtain a good adhesive seal.
- If required, use barrier film, stoma paste or powder to protect the skin and manage leaks.
- If required, shave hairy areas once a week using a clean razor.
- Use medical adhesive removers to gently lift the adhesive on removal, to avoid skin trauma and stripping.
- Refer to local stoma care nurse specialist for assessment, advice and support.
(Cowell, et al. 2011. Al-Niaimi et al. 2012. Schuetz & Sanchez, 2023)
In conclusion, both Peri-wound and Peristomal dermatitis present several clinical challenges and management will require clinicians to have a greater understanding of what it is, the causes, signs and symptoms, and how to manage these to help prevent and effectively manage these conditions. This starts with a patient-centred, holistic, and problem-solving approach alongside adopting a structured skin care regime to cleanse and protect the skin which should be reflected in the care plans available to all staff. The importance of clear, interprofessional communication, clear care guidelines and seeking further advice if interventions are key to achieving a positive outcome.
More blogs on MASD:
Under the Umbrella of MASD – Intertriginous Dermatitis (ITD)
Under the umbrella of MASD – Incontinence Associated Dermatitis (IAD)
References
Al-Niaimi et al. (2012). The relevance of patch testing in peristomal dermatitis. British Journal of Dermatology. Vol 167 (1). Pg 103-109
Collier, M. Simon, D. (2016) Protecting vulnerable skin from moisture-associated skin damage. British Journal of Nursing. Vol 25 (20). bjon.2016.25.20.S26
Colwell, J. C., et al. (2011). MASD Part 3: Peristomal Moisture-Associated Dermatitis and Periwound Moisture-Associated Dermatitis. J Wound Ostomy Continence Nurse. Vol 38 (5). Pg 541-553. https://nursing.ceconnection.com/ovidfiles/00152192-201109000-00011.pdf
Dowsett C, Protz K, Drouard M, Harding KG. (2015a). Triangle of wound assessment. Wounds International. Available at https://www.woundsinternational.com/ Accessed 11/10/23
Dowsett, C. and Allen, L. (2013). Moisture-associated skin damage made easy. Wounds UK 94(4). Available from www.wounds-uk.com/made-easy. Accessed 11/10/23.
Holloway, S. (2019). Skin considerations for older adults with wounds. British Journal of Community Nursing. Vol 24 (sup 6). bjcn.2019.24.Sup6.S15
Holloway, S. (2020). Peri-wound skin care considerations for older adults. Practice Nursing. Vol 31 (8). Accessed 11/10/23 available at pnur.2020.31.8.326
Mitchell, A. Hill, B. (2020). Moisture-associated skin damage: an overview of its diagnosis and management. British Journal of Community Nursing. Vol 25(3). bjcn.2020.25.Sup3.S12
Schuetz, S. J., Sanchez, M. (2023) Preventive stoma care and peristomal skin conditions. Seminars in Colon and Rectal Surgery, Vol 34 (2). https://doi.org/10.1016/j.scrs.2023.100959
Image sources
Fig 1 – Hampton, S. (2019) Macerated foot. Taken from BLOG What is Maceration? https://oska.uk.com/what-is-maceration/