Heel pressure ulcers: anatomical vulnerability, risk factors, and preventive strategies
This article highlights the risk for the development of heel pressure ulcers and the second part in this series will summarise the new 2025 NPIAP/EPUAP Guidelines for Preventing Heel Pressure Ulcers.
Introduction
Pressure ulcers (PUs) remain a major challenge in healthcare, particularly among immobile and critically ill patients. The heel is the second most common anatomical site for PUs and is considered highly vulnerable due to its unique structural and physiological characteristics (Delmore & Ayello, 2021). Understanding the anatomical predisposition, associated risk factors, and evidence-based preventative strategies is essential for improving patient outcomes and reducing healthcare costs.
The heels’ susceptibility to pressure injuries is primarily due to its minimal soft tissue coverage and the presence of the calcaneus, a rigid bone which is only covered by a thin layer of skin and subcutaneous tissue (Greenwood, 2022). The posterior aspect of the heel lacks muscle or fascia, which limits its ability to cushion pressure (Gefen et al., 2018). When patients lie on their back, the heel often bears significant pressure, especially if the foot is dropping forward (plantarflexion), which causes the heel rim to come into contact with the support surface (Haesler, 2017). This pressure is exaggerated by shear forces which can occur during repositioning or unintended/ involuntary movement, which can damage deep tissue structures (Gefen et al., 2018).
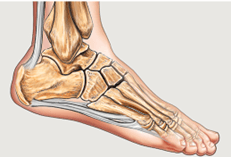
Fig.1. Nucleus Medical Media Inc / Alamy Stock Photo
Risk factors
Several intrinsic and extrinsic factors increase the risk of heel PUs. Intrinsic (internal) factors include ageing and associated skin changes, diabetes mellitus, peripheral vascular disease, and neuropathy, all of which have an impact on a patient’s tissue perfusion and ability to feel pressure or pain (Delmore & Ayello, 2021). Fat pad atrophy in older adults further reduces the cushioning capacity of the heel (Greenwood, 2022).
Extrinsic (external) factors include immobility, long surgical procedures without adequate heel offloading, inadequate repositioning including during prolonged diagnostic or therapeutic interventions, epidurals, heavy sheets/duvets pressing on the feet, splints for foot drop, Plaster of Paris (POP), as well as heels resting on stools while sitting out (Haesler, 2017).
Preventive strategies
Evidence-based guidelines emphasise a multifaceted approach to prevention. The EPUAP International Guidelines recommend regular risk assessment, skin inspection, and the use of pressure redistribution surfaces (NPIAP/EPUAP, 2019). Offloading the heel completely using offloading devices, such as booties, pillows or mattresses with heel Offloader foam (e.g. OSKA Series2 or OSKA Series4 or OSKA Series4H), or positioning techniques, such as using the knee break facility on an electric profiling bed, significantly reduces PU incidence (Haesler, 2017). Additional interventions include maintaining optimal skin microclimate, avoiding friction and shear, and ensuring adequate nutrition and hydration (Al-Qudimat et al., 2024).
Discussion and conclusion
Despite advances in prevention, heel PUs continue to be a problem, particularly in high-risk populations such as immobile or critically ill patients. A recent cohort study found that even with preventive protocols, 22% of PUs occurred on the heel, highlighting the need for individualised care plans and adherence to best practices (Martín-Meana et al., 2025).
The heel’s anatomical structure and limited tissue protection make it highly susceptible to pressure ulcers. Risk factors such as immobility, vascular impairment, and sensory deficits further exacerbate vulnerability. Preventive strategies should prioritise heel offloading, regular repositioning, and comprehensive risk assessment.
Please cite as: OSKA Care Ltd. (January 2026). Heel pressure ulcers: anatomical vulnerability, risk factors, and preventive strategies. Havant, Portsmouth: OSKA Care Ltd.
References
- Al-Qudimat, A. R., Maabreh, A. H., Shtayat, H., Khaleel, M. A., Allatayfeh, J. M., & Iblasi, A. S. (2024). Prevention of pressure injuries and nursing interventions in critical care settings: A synthesis without meta-analysis. Chronic Wound Care Management and Research, 11, 13–30. https://doi.org/10.2147/CWCMR.S434625. Accessed 05.12.25
- Delmore, B., & Ayello, E. A. (2021). Heel pressure injuries. Advances in Skin & Wound Care, 34(5), 236–237.
- Gefen, A., Brindle, C., Black, J., Santamaria, N., & Alves, P. (2018). Prevention and management of pressure injury to the heel. Wounds International. Available at https://woundsinternational.com/journal-articles/prevention-and-management-of-pressure-injury-to-the-heel/ (accessed 28.11.25)
- Greenwood, C. (2022). Heel pressure ulcers: Understanding why they develop and how to prevent them. Nursing Standard, 37(2), 60-66. Accessed 05.12.25.
- Greenwood, C., Nelson, E. A., Nixon, J., Vargas-Palacios, A., & McGinnis, E. (2022). Comparative effectiveness of heel-specific medical devices for the prevention of heel pressure ulcers: A systematic review. Journal of Tissue Viability, 31(5), 579–592.Available at https://pubmed.ncbi.nlm.nih.gov/36272951/. Accessed 05.12.25
- Haesler, E. (2017). Evidence summary: Pressure injuries: Preventing heel pressure injuries with positioning. Cambridge Media Journals. Available at https://journals.cambridgemedia.com.au/wpr/volume-25-number-4/evidence-summary-pressure-injuries-preventing-heel-pressure-injuries-positioning (accessed 28.11.25)
- Martín-Meana, C., González-Darias, J. M., Chinea-Rodríguez, C. D., et al. (2025). Effectiveness of additional preventive measures for pressure injury prevention in an intensive care unit: A retrospective cohort study. Nursing Reports, 15(7), 259. https://doi.org/10.3390/nursrep15070259. Accessed 05.12.25
- National Pressure Injury Advisory Panel (NPIAP). (2019). Prevention and treatment of pressure ulcers/injuries: Clinical practice guideline. Available at https://epuap.org/pu-guidelines/